The lockdown has taken away many of our social and leisure opportunities, restricted our travel and our ability to teach and learn in a natural, face-to-face environment. As we struggle to find the headspace to work and draw virtual lines to separate or home and work lives, a few welcome gifts have arrived.
Many companies have provided free or extended access to their online resources such as video streaming services, kids education resources and learning software.
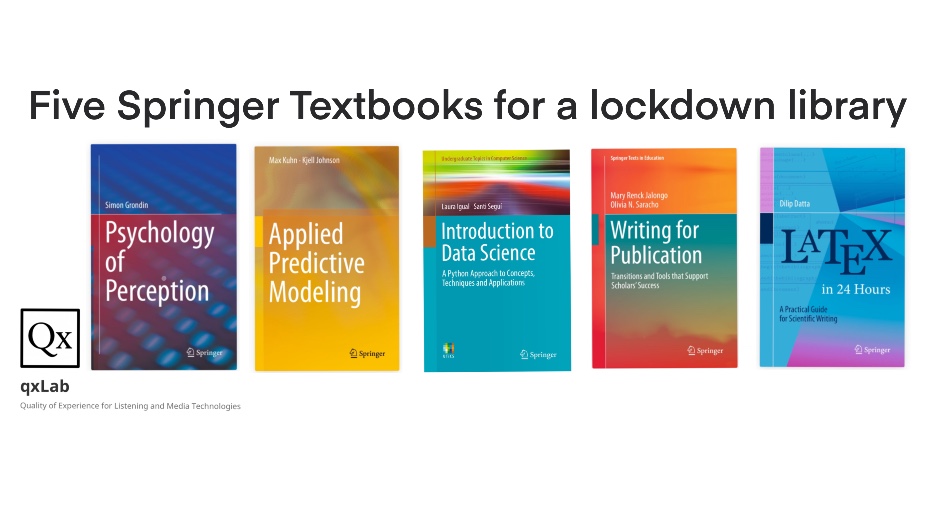
From an academic perspective, the Springer book series that has been made available has provided a new bookcase on my tablet of introductory texts across a range of topics. After a discussion on our lab group #random slack channel, a few books were suggested so I’ve put together a post of the top picks.
For those interested in working in the area of Predictive Modelling for Multimedia Quality of Experience, I’ve put together a top 5 books bootstrap your productivity. New PhD students at QxLab will find this a good place to start.
Psychology of Perception: This book the terminology used in perception and the biological and physical bases required for understanding sensory experiences. The chapter on hearing introduces speech and audio perception touching on phonemes, psychoacoustics and musical notes.
Applied Predictive Modeling: The different ways of implementing regression and classification models are presented. Chapter 20 is a nice introduction to the factors that can affect model performance, highlighting how models may predict something other than the factor you expect.
Introduction to Data Science: Getting familiar with the syntax and libraries of Python, Pandas, Numpy and Scipy through Jupyter Notebooks. Data understanding, preparation and wrangling is the foundation of any good data-driven model so this book gives a good crash course. Especially useful if you come from a MATLAB background and want to get up to speed with Python.
Writing for Publication: Procrastination, aversion to writing, uncertainty and fear of criticism impact us all throughout our research careers so any book that deals with these in chapter one before getting into the difference between conference and journal publications seems good to me. From the benefits of collaborative authorship, to dealing with editors it has a lot of nice tips regarding academic writing that go beyond the concrete advice on first drafts, titles, abstracts etc. which are also covered.
LaTeX in 24 Hours: Learning to use LaTeX is the best way to increase the efficiency of academic writing. Managing citations with BibTeX beats word any day, but using Overleaf for collaborative authoring, commenting and markup for revisions and version control makes it the markup language of academic writing. I never had a book on LaTeX and as with anything the you learn as you go, it is nice to be able to dip in and see chapters containing simple things you’ve never come across before (e.g. chapters 17 and 18 has lots about boxes).
I’ve saved these to iBooks on my iPad so next time I’m looking for a book to browse I have several options at hand.
The paper pulls together all of the subjective QoE experimental work conducted during his PhD research and explores the relationship between different audio and video quality issues and how they influence quality when they interact.
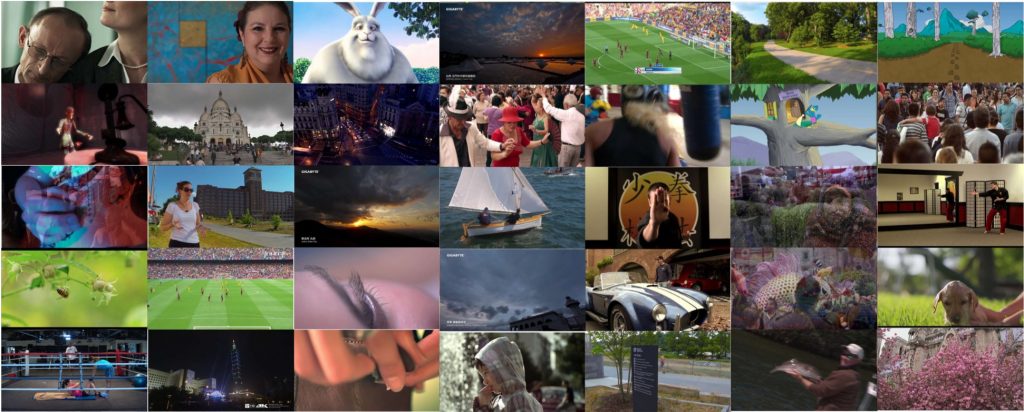
UnB-AV: An Audio-Visual Database for Multimedia Quality Research
The paper describes an open research database of audio-visual sequences and quality scores aimed at multimedia quality research. The database contains a total of 140 source content, with a diverse semantic content, both in terms of the video and audio components. It also contains 2,320 test sequences with audio and video degradations, along with the corresponding quality and content subjective scores. The subjective scores were collected by performing 3 different psycho-physical experiments using the Immersive Methodology. The three experiments have been presented individually in previous studies. In the first experiment, only the video component of the audio-visual sequences were degraded with compression (H.264 and H.265) and transmission (packet-loss and frame freezing) distortions. In the second experiment, only the audio component of the audio-visual sequences were degraded with common audio distortions (clip, echo, chop, and background noise). Finally, in the third experiment the audio and video degradations were combined to degrade both audio and video components. The UnB-AV database is available for download from the site of the Laboratory of Digital Signal Processing of the University of Brasilia and The Consumer Digital Video Library (CDVL).
I spent a lot of the last couple of weeks in bed with an undiagnosed respiratory illness that may or may not have been COVID, so I was not up to doing much other than browsing twitter from time-to-time. I was curious about the research, highlighted by Luke O’Neill and others potentially linking susceptibility to COVID and national BCG vaccination policies.
My first thought, based on a colleagues tweet, was to be wary of thinking you can do epidemiology research.
Yes. Be careful of the “infectious disease epidemiology – how hard can it be” trap. https://t.co/XSp9oFoCqy
Ignoring the wise advice, and driven by curiosity, I decided to bootstrap some code from Barry Smyth and compare the European Centre for Disease Prevention and Control and the BCG world atlas to see if any trend could be visualised.
The results were interesting enough to me to write up and share, although, with the strong caveat that this was a rough exercise by a convalescent non-expert!
Background
The Covid-19 pandemic has resulted in over 1.3 million infections and 300,000 deaths 80,000 deaths between January and the 8th April 2020. Recently published papers suggest vaccination with Bacillus Calmette-Guérin (BCG) could have protective effects against viral infection. BCG has been in use since 1921 [1] and is a safe vaccine that has been shown in some trials to provide some level of protection for other a wide range of pathogens including viruses [2]. A number of randomised clinical trials have begun to investigate whether the BCG vaccine is playing a contributory role in suppressing the COVID-19 pandemic spread [3]. There has been speculation that a higher blanket immunity among the young could be providing a shield for the elderly in some countries, reducing the pandemic mortality rates~\cite{irishtimes2020}. In the interim, studies of the rates of mortality in the population could allow a better population based understanding of potential contributory factors. Zafirakis et al. [4] and [5] examined whether a relationship could be identified between national BCG vaccination programs and the mortality levels reported by countries.
Inspired by Shet et al. [6] who reported a COVID-19-attributable mortality among BCG-using countries as 5.8 times lower [95\% CI 1.8- 19.0] than in non BCG-using countries, this work sought to use existing data and visualisations with a simple linear regression model to illustrate this finding using only the raw daily cases and death statistics statistics and comparing for countries with different BCG vaccination policies.
Data Sources and Preparation
Daily cases and death statistics attributed to Covid-19 was sourced from the European Centre for Disease Prevention and Control. Per country BCG vaccination policy classifications was retrieved from the World Atlas of BCG [7]. The data was processed using scripts based on scripts from Barry Smyth developed to plot visualisations of daily cumulative cases and deaths inspired by the excellent daily update visualisations produced by John Burn-Murdoch of the Financial Times.
The BCG World Atlas categorised the database of policies and practices of the Bacillus Calmette-Guérin (BCG) vaccine from countries all over the world with details on the changes in policy over time. At a high level there are three main country policies: (a) Current national BCG vaccination policy for all; (b) Past national BCG vaccination policy for all; and (c) BCG recommendation only for specific groups or none at all.
More stratified categories from [7] based on the policy commencement year, subset of populations vaccinated, etc. are not considered here. Many other factors such as those considered in the modelling of [6] or other factors such as the levels of immigration, wealth, vaccination take-up and healthcare systems could also play a factor but are not considered.
Rate of increase in Cases and Deaths
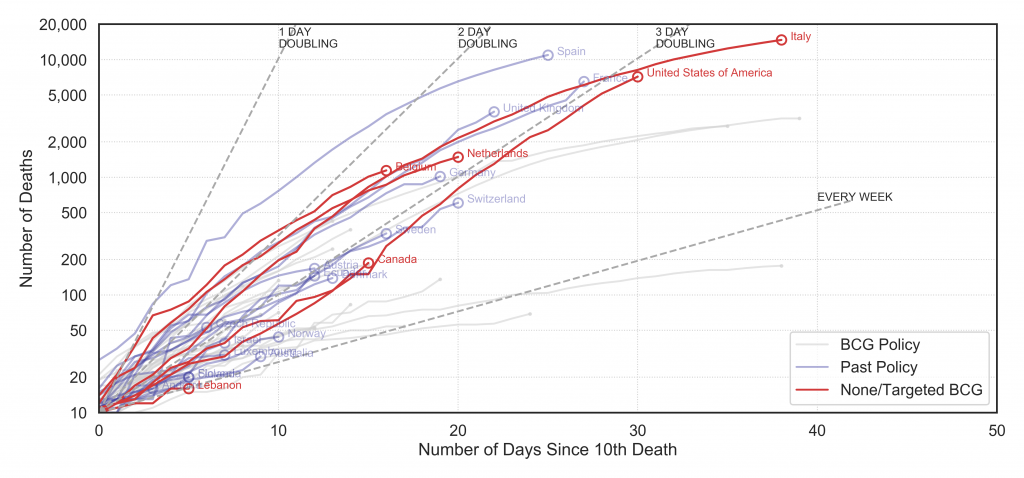
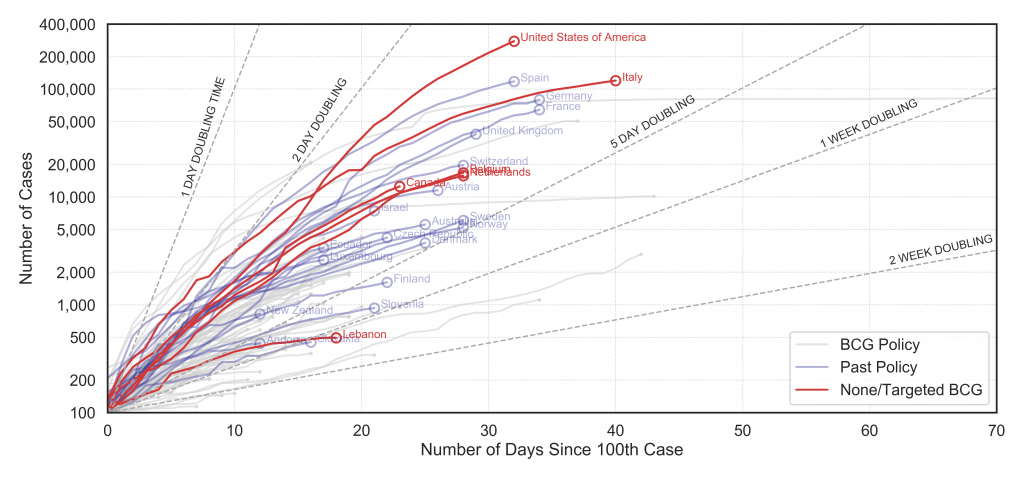
The cumulative cases and deaths per country are plotted, colour-coded by BCG policy class in Fig. 1 and Fig. 2. Both graphs plot the cumulative number of cases per day with a log scaled y-axis. The grey dashed lines show what a trend following an exponential doubling of cases per day, two days etc. would follow. They are plotted from day zero when 100 cases identified in Fig. 1 and 10 deaths occurs in Fig. 2.It should be noted that the reporting on cases varies by country and even within countries as the testing criteria, protocol and capacity change. Hence the daily cases should be treated as unreliable.
Figure 1: Daily cumulative cases by country starting from 100 cases (Data to: 4 Apr 2020)
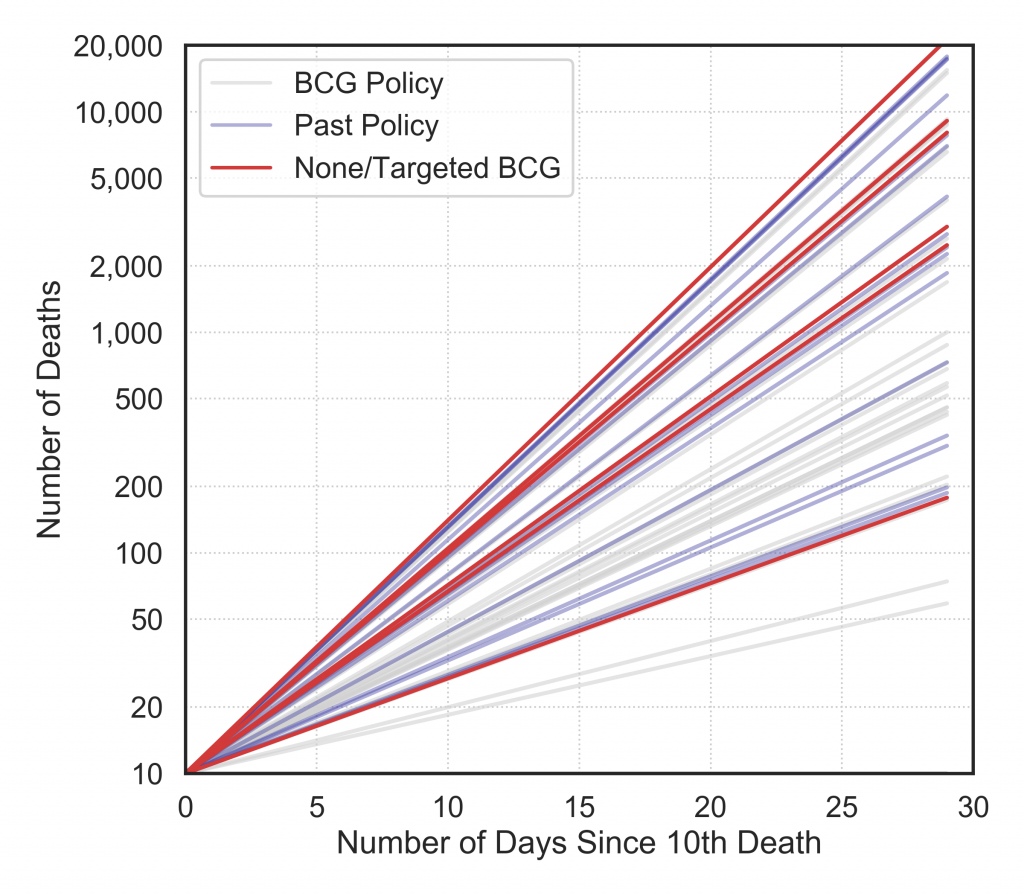
Figure 2: Daily cumulative deaths by country starting from 10 deaths (Data to: 4 Apr 2020)
In Fig. 2, the cumulative deaths reported are plotted. This data has some of the same quality issues, e.g. deaths outside hospitals are delayed in reporting, are mis-classified or are reported in bulk on a lagging timescale. However, it can be considered better than the cases data in terms of quality.
Looking at both graphs there is a sense that there is a trend that the red and blue lines (i.e. classes with less or no vaccination) are following steeper trends than the grey lines but it is difficult interpret.
Rate of increase in Cases and Deaths
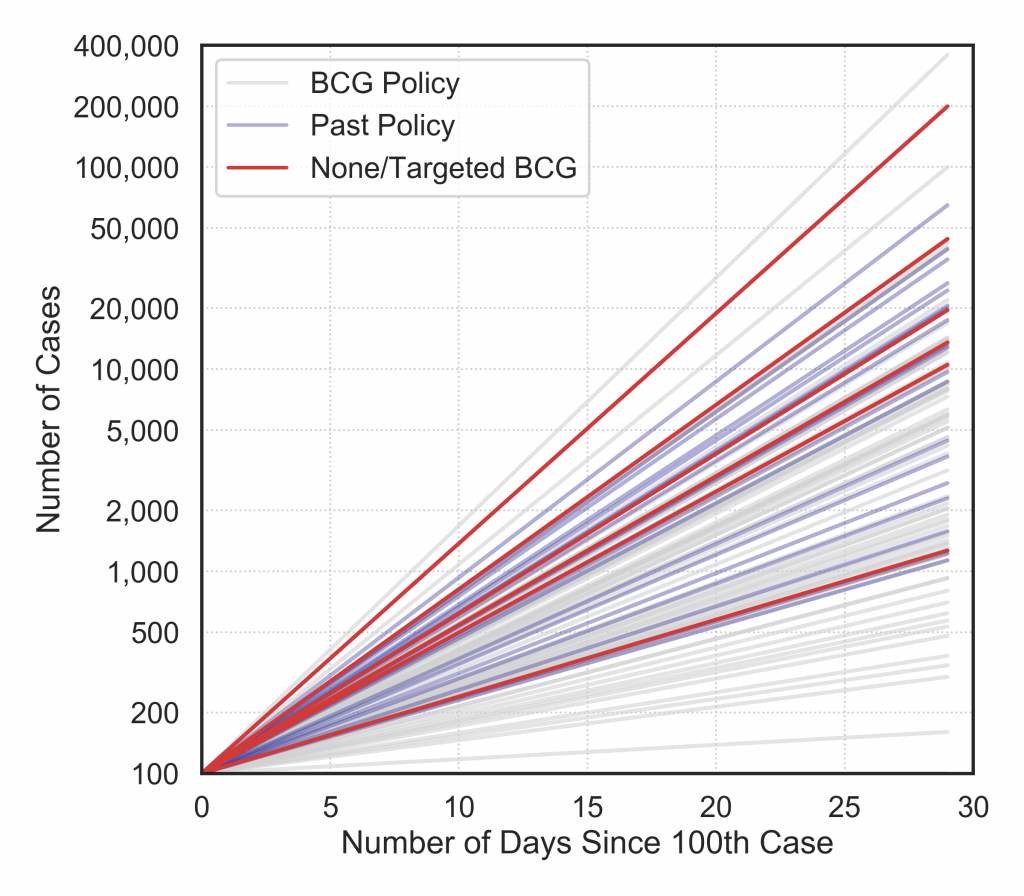
In order to compare across countries in a consistent manner, the maximum slope of the cumulative cases and deaths per country are computed as a linear regression fit over 5 day windows. This gives an indication of the peak rise in cases and deaths. These are plotted in Fig. 3.For both a trend emerges in the red and blue lines (None/Targeted BCG and Past Policy) having steeper trajectories. The outliers are countries like Lebanon and Andorra with relatively low numbers of cases and deaths reported to date.
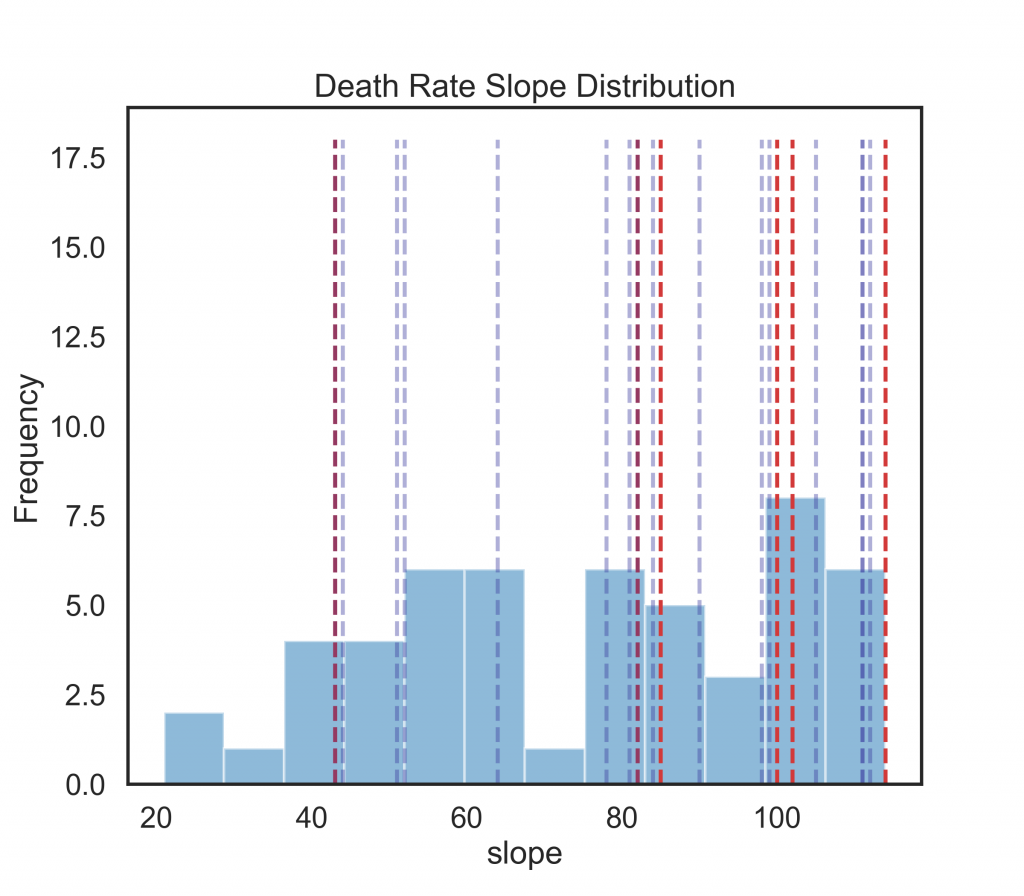
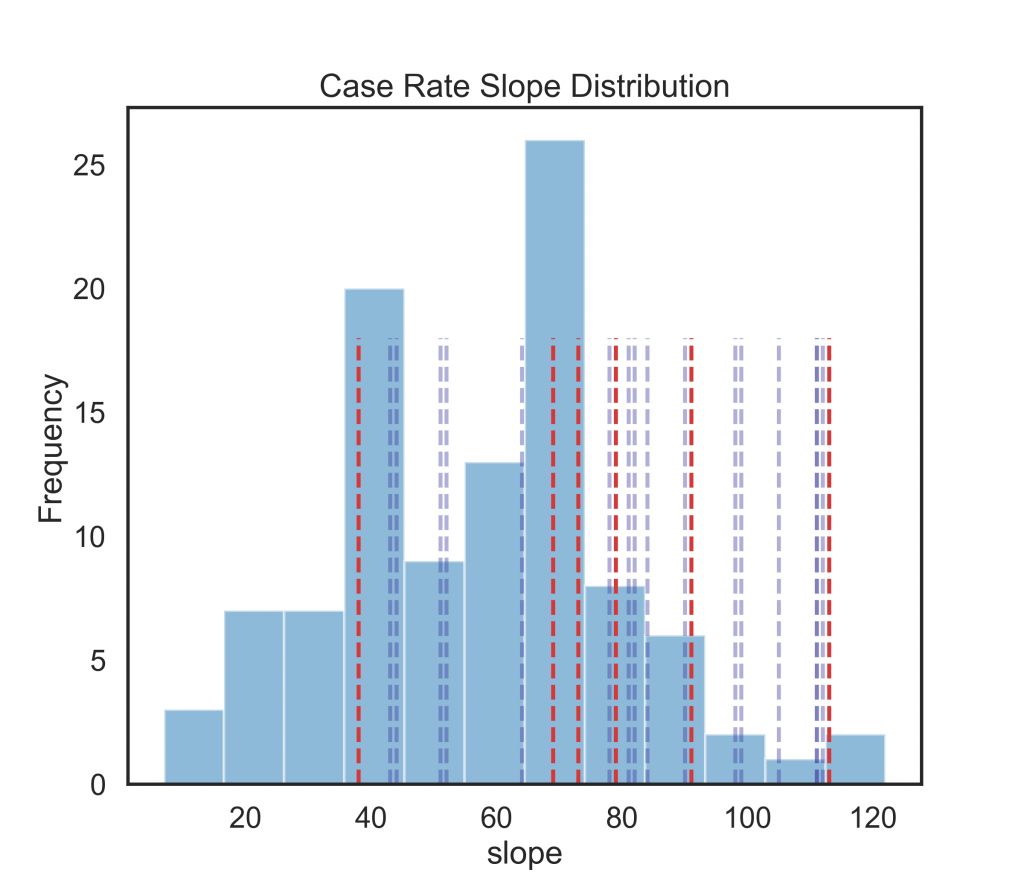
This data is also visualised in Fig. 4 where the full distribution of slopes are plotted in a 12 bin histogram and dashed lines indicate the slopes of the countries outside of full population vaccination class (a). Again, the cases are noisy but do illustrate the skew. The deaths highlight that all the dashed red lines except one outlier (Lebanon) lie in the top third of the peak slope distributions.
Figure 3: Maximum slope of 5-day sampled linear regression of cumulative daily cases by country.Figure 4: Maximum slope of 5-day sampled linear regression of cumulative daily deaths by country. The majority of the red and blue lines have a steeper slope than the grey lines for countries with a national BCG policy.
Figure 5: Histogram showing the maximum slope distributions for countries cumulative cases. The red lines show the individual country maximim slope rates for countries with None/Selective BCG vaccination policies; blue dashed lines are countries with past polices.Figure 6: Histogram showing the maximum slope distributions for countries cumulative daily deaths. The red lines show the individual country maximim slope rates for countries with None/Selective BCG vaccination policies; blue dashed lines are countries with past polices.
Conclusions
It may be simplistic to draw too much from a simple linear regression maximum slope over 5 days analysis. However, the daily COVID-19 case and death statistics reported show a correlation trend with national BCG vaccination policies that is similar to the findings reported in [6]. Followup analysis when the countries that are still in the earlier stages of the pandemic report further cases and mortality may clarify whether the outliers are due to noisy data or significant factors.
References
World Health Organization. BCG vaccine: WHO position paper, February 2018 – recommendations. Vaccine, 36(24):3408–3410, Jun 2018.
Jop Vrieze. Can a century-old TB vaccine steel the immune system against the new coronavirus? Science, Mar 2020.
David Alnwick. Letter to the editor: Struggling to combat Covid-19. The Irish Times, 7 Apr 2020.
Helen Zafirakis Andrew DiNardo Paul K. Hegarty, Ashish Kamat. Bcg vaccination may be protective against covid-19. ResearchGate Preprint, 2020.
Elisabeth Mahase. Covid-19: what treatments are being investigated? BMJ, page m1252, Mar 2020.
Anita Shet, Debashree Ray, Neelika Malavige, Mathuram Santosham, and Naor Bar-Zeev. Differential covid-19- attributable mortality and bcg vaccine use in countries. medRxiv, 2020.
Alice Zwerling, Marcel A Behr, Aman Verma, Timothy F Brewer, Dick Menzies, and Madhukar Pai. The BCG world atlas: a database of global BCG vaccination policies and practices. PLoS medicine, 8(3), 2011.